

Many pregnant individuals are curious about the immediate effect of delivering a baby vaginally. Many have heard stories about getting “cut” during the delivery or needing stitches for tearing. In fact, having a tear is common, with up to 80% of individuals experiencing a tear at the time of a vaginal birth. In this article you will learn about:
- The types of tears that can occur during a vaginal delivery
- What an episiotomy is
- How obstetric tears are repaired
- Ways to lower your chance of having a tear during your delivery
- The risk of tears with future births
What types of tears can occur during a vaginal delivery?
The vulva is a general term to describe the outside female genital structures. The vulva includes the labia majora and minora, mons pubis, clitoris, vaginal vestibule, and the perineal body. Each of these area can be injured during childbirth.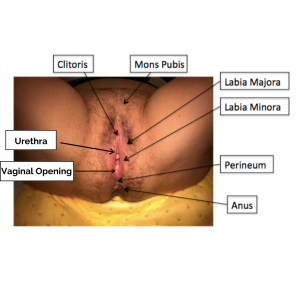
The perineal body, which is the space between the vaginal and anal openings, is the most common site to tear during childbirth. It is made up of the vulvar skin, vaginal lining, several muscles, and connective tissue. A classification system was developed to describe the severity of a perineal tear. It ranges from 1st to 4th degree based upon the structures involved. Each degree of tear builds upon the previous one and they are increasingly more severe.
- 1st degree: A tear to the perineal skin only
- 2nd degree: A tear into the perineum involving the underlying muscles
- 3rd degree: A tear into the muscles surrounding the anus, also known as the anal sphincters
- 4th degree: A tear into the anus and/or rectum
The majority of tears are classified as 1st or 2nd degree. Only a small percent of individuals (<5%) have the more severe 3rd and 4th degree tears, which are commonly referred to as obstetric anal sphincter injuries (OASIS).
It is also possible to have a tear on either the labia majora and/or labia minora. Sometimes people have a tear near the urethra or clitoris. If these are not bleeding, they are often not repaired because the stitches can be irritating in these sensitive areas. It is also possible to have tears that just occur in the vagina. In rare instances, there can be a tear in the cervix. These areas may or may not require stitches depending upon the size and severity of the tear, as well as if bleeding is occurring.
What puts a person at risk for OASIS?
There are certain things that put a person at increased risk for OASIS, or a 3rd or 4th degree tear. It is easiest to classify these factors in two ways:
- “inherent”- those that a person cannot change
- “modifiable”- those related to a specific situation in the delivery.
Inherent risk factors that increase an individual’s risk of having an OASIS include:
- Having one’s first vaginal delivery
- Being of Asian ethnicity
- Having a family history of OASIS in one’s mother or sisters
- Having a short distance between the vagina and anal opening
- Delivering a large baby, weighing more than 8 pounds
Modifiable risk factors for OASIS include:
- Needing help to deliver the baby, either with a vacuum (a suction cup device that the obstetric provider places on the top of the baby’s head) or forceps (blunt metal blades that are placed alongside the baby’s cheeks). These devices are generally used to speed up delivery if there are concerns about the baby’s well-being or if the birthing person is exhausted from pushing for a long time.
- Episiotomy, especially when performed in the middle of the perineum
- If the baby delivers face up. This is because the distance around the head is larger than if the baby tucks its chin down towards its chest and is coming out face down. Delivering face up is less common than face down.
- Pushing for a long period of time.
What is an episiotomy and why are they performed?
An episiotomy is an intentional cut in the perineum at the vaginal opening made by the obstetric provider. These cuts are used to create more space to deliver the baby’s head. Episiotomies were performed more frequently in the past. Due to their association with OASIS, they are used most commonly in situations when there is difficulty with getting the baby out, if the vulvar skin is preventing the head from delivering, or if delivery needs to be quickened.
There are two main types of episiotomies:
- A median episiotomy is when a cut is made in the middle of the vaginal opening. These are linked to increased OASIS, as the cut can spread down the perineum to the anal sphincter.
- A mediolateral episiotomy is when the cut is made off to the side of the vaginal opening. These are associated with more bleeding and may hurt more.
How are tears repaired?
If tears are not bleeding a lot and do not significantly change the way a person’s vulva looks, they may not need any stitches. This includes first degree tears and other small tears of the vulvar structures, as previously described. When a repair is needed, small sutures that dissolve on their own over time are typically used. Sometimes for small tears, a surgical skin glue can be used. Often a provider will use one long stitch to bring the tissue back together. However, sometimes several individual stitches may be used as well. Many of the stitches may be underneath the skin and not visible. The majority of tears can be fixed in the delivery room, using either numbing pain medicine or the epidural medicine if an individual already has one.
Some larger tears may need to be repaired in the operating room. Someone might need their tear repaired in the operating room if there is increased bleeding or if the person needs extra measures to have good pain control. In the operating room, the obstetric provider can have better lighting, get the person in a better position, and have more equipment. Together, these things can make it easier to perform the repair. If a person has an OASIS, IV antibiotics may be given at the time of the repair.
What are the complications related to tears?
The majority of individuals with a tear from a vaginal birth will heal with time and have no problems. There are, however, several problems that can occur after a tear. These include:
- Bleeding: This is the most common issue. It can often be stopped by holding pressure, for example with a surgical sponge, or with additional stitches.
- Infection of the tear: This most commonly occurs after OASIS. A person may notice a foul-smelling, pus-like discharge, and it may be associated with increased pain. If a person thinks there may be an infection after delivery, they should contact their obstetric provider. These infections can generally be treated with antibiotics taken by mouth. If an infection occurs, it is also important to perform good perineal care. This means keeping the area as clean and dry as possible. Pad changes should be performed frequently. The area can be cleansed with warm water. Sitz baths should be performed up to three times per day. These measures will help encourage healing.
- Pain: Most people experience pain or soreness after having a vaginal birth, even if no tear is present. Most of the time, a person can have control of this discomfort using over the counter medications, such as acetaminophen or ibuprofen. There are also over the counter topical numbing sprays and ointments that can be used directly on the area that hurts. Ice packs applied for no more than 20 minutes at a time can provide relief of discomfort. For most people, the pain is gone by 3 weeks after delivering.
- Breakdown: This is when the stitches separate and the wound opens back up. Overall, this happens in only a small number of people, less than 1 in 20. Individuals who have an OASIS, however, are at higher risk for this happening. Sometimes this can happen if there is an infection of the tear. If a person thinks that their tear has opened, they should contact their obstetric provider to have their bottom examined. Perineal care, as described above, and sitz baths are helpful for healing. Some breakdowns may need to be surgically fixed at a later time if they do not heal on their own or if they significantly alter the normal anatomy.
- Pain with sex: It is not uncommon for sex to be uncomfortable the first couple of times after having a baby. However, this discomfort generally lessens with time. For parents who breastfeed, the change in hormones can also cause vaginal dryness. After an OASIS, however, it is more common to have pain with sex. Many people who have an OASIS do not have sex until several weeks later than individuals who have smaller tears. This is because healing can take longer. Techniques to help with discomfort include foreplay, perineal massage, and utilizing lubrication, such as organic coconut oil or water-based lubricants. If the discomfort does not go away or a person is concerned about the discomfort, they should discuss this with their obstetric provider.
- Bowel control issues: This can include having the sensation of needing to get to the bathroom quickly as soon as there is an urge to have a bowel movement, passing gas without being able to control it, or leaking stool. These issues most commonly occur when a person has an OASIS. For the majority of people who experience bowel control issues after delivery, these will improve with time and resolve once the tear has fully healed. Some people will need to go to specialized physical therapy to help improve the strength of the vaginal and pelvic muscles. If a person has issues with bowel control, they should contact their obstetric provider.
What is a sitz bath?
A sitz bath involves soaking the bottom for 10 minutes at a time, two to three times a day. These can be very helpful to promote healing. The person should choose the temperature of the water that is most comfortable. Epsom salts can be added if desired, but are not necessary. Some hospitals provide sitz baths that can be used with the toilet. A bathtub can also be used, with a couple inches of water. After a sitz bath, the person’s bottom should be patted dry with a clean towel or a hair dryer can be used on a cool setting.
How can someone reduce the risk of having a tear?
Several techniques have been suggested to help reduce the risk of having a tear. Unfortunately, only small reductions in tearing has been shown. One technique associated with reducing tear risk is perineal massage performed by the pregnant person. This should be started at 34 weeks of pregnancy and continued regularly until delivery. The massage can also be performed while the person is pushing. In studies, perineal massage prevented 1 tear out of 10 people. Some researchers have suggested that holding support on the perineum while the baby’s head is delivering can lower the chances of tearing. Other researchers have found that this is not helpful. Applying warm compresses to the perineum during labor and pushing may reduce the risk of tearing. There may also be a small benefit to pushing on one’s side during delivery.
 What are the chances of having a tear again in the future?
What are the chances of having a tear again in the future?
Oftentimes people labor and push for a shorter amount of time with future vaginal births. Some people who had a small tear during their first birth have no tear with deliveries thereafter. Others may have the same degree of tear or a lesser tear. For people with the most severe tears, OASIS, the chance of having another OASIS is only 3-8%, which means that the majority of people (more than 9 out of 10) will not have another severe tear of this type.
Are there tears that would prevent a person from having a vaginal birth in the future?
The majority of people who have had a tear will go on to have another vaginal birth in the future. For some people who have OASIS, a cesarean section may be recommended if:
- bowel control issues are present after delivery
- there are wound complications like infection or breakdown, or
- if the person expresses psychological distress from their delivery.
If a person is unsure as to whether or not they should have a vaginal delivery, they should have a discussion with their obstetric provider. Their provider can explain the pros and cons of future vaginal births, reviewing the risk factors that could change (“modifiable”) versus those that are unique to the person. While shared decision making is helpful, it is ultimately the birthing person’s choice if they would like to try for a vaginal delivery in the future. There are only a small number of situations where the obstetric provider would say it is unsafe to have another vaginal birth.
Take Home Points
- Most pregnant people have a tear at the time of their first vaginal birth, but they are usually small.
- The tears can occur in any of the vulvar structures, but most commonly occur in the perineum. These tears are on a scale of 1st to 4th degree.
- While the majority of people heal normally after a vaginal delivery, there are some problems and complications that can occur.
- The majority of people are able to have another vaginal birth after their initial birth and may experience the same or a lesser tear.
Author Information

Lisa Hickman, M.D. graduated from the Ohio State University College of Medicine. She completed her residency in Obstetrics and Gynecology at the Cleveland Clinic and is currently a fellow in Urogynecology and Reconstructive Pelvic Surgery at the Cleveland Clinic. She has a special interest in the impact of childbirth on the pelvic floor.
No conflicts of interest to report.

